
I recently attended the Mayo Clinic's continuing medical education seminar on Collaborative 3D Printing in Medical Practice. I have been closely following the news on the early efforts to adopt additive manufacturing (AM) techniques in the hospital setting and have recently sensed an uptick in the frequency of use (and frankly the utility) of the technology. One of the best features of the conference was that the speakers were so thoughtful, unmistakably enthusiastic about 3D printing and its value, and were open to sharing their time and considerable experience with the attendees.
There are some amazing things being done using 3D printing by the surgeons at the Mayo Clinic and other institutions around the country. There were several times that I was sitting in the audience thinking, I don't follow national surgeon rankings, but I know this person is the Michael Jordan of what they do.
While 3D printing in the medical context started out helping doctors visualize surgical cases that were truly corner cases (like the separation of conjoined twins at the Mayo Clinic), there is also much evidence that more routine surgical procedures benefit from the fact that 3D imaging and printing allows for the creation of patient-specific visualization tools, surgical guides, templates and as they would say in the carpentry world "jigs." I will discuss some of those clinical applications below.
There are some amazing things being done using 3D printing by the surgeons at the Mayo Clinic and other institutions around the country. There were several times that I was sitting in the audience thinking, I don't follow national surgeon rankings, but I know this person is the Michael Jordan of what they do.
While 3D printing in the medical context started out helping doctors visualize surgical cases that were truly corner cases (like the separation of conjoined twins at the Mayo Clinic), there is also much evidence that more routine surgical procedures benefit from the fact that 3D imaging and printing allows for the creation of patient-specific visualization tools, surgical guides, templates and as they would say in the carpentry world "jigs." I will discuss some of those clinical applications below.
Current state of 3D printing in hospitals
So, who is doing what with 3D printing in the hospital context? Since there was not a readily available list of participating institutions, I prepared a list of hospitals in North America that have 3D printing programs. Many of the best names in clinical care are on the list of 40 institutions. While I'm sure there are others, here is a sampling of who is involved.
I have included a more comprehensive list at the end of this article (based on what I could find from public news sources) which includes information on the types of 3D printer used by each program, the medical departments involved and the clinical applications described in news stories about the program.
Clinical Applications of 3D Printing in Surgery
So, how is 3D printing being used today? It spans the gamut from helping nearly 30 doctors and operating room personnel to visualize and communicate about the complex process of separating conjoined twins (as done in 2006 at the Mayo Clinic) to a more routine use as an orthopedic custom cutting guide for knee replacement surgery.
Cardiothoracic surgeons are now using 3D printed heart models with increasing frequency, particularly for pediatric cases. They use the models for pre-surgical planning, intraoperative visualization and even for training and technique practice using models printed with flexible, almost realistic material properties. Another use case involves planning and simulation of complex endovascular aortic repair. Surgeons use models to better plan for cases of Arteriovenus malformations (AVM) and cases involving ventricular septal defects (a hole in a wall of the heart). They are also using models to pre-plan and practice transcatheter valve positioning and for heart valve replacement planning. In a discussion of the use of 3D printing in cardiothoracic surgery, Dr. Stephen Cassivi of the Mayo Clinic described what he referred to as "the power of touch" and how these models can enhance the surgeon's understanding of complex or unusual anatomy. In fact, several surgeons mentioned the concept of "If I touch it, I own it."
A well publicized life-saving use of 3D printing technology involved the University of Michican CS Mott Children's Hospital's use of an implantable, bioresorbable splint for a young boy's tracheo-bronchomalacia (thinning of the wall(s) of the airway). The surgeons sought and received emergency approval from the FDA to use a 3D printed splint that used materials that would be resorbed into the patient's body over the course of several years but in the mean time would act as a scaffold on which the patient's own cells could regrow. This case is at the intersection of what I think of as the now of medical 3DP and its future. The future of medical 3DP is expected to involve the 3D bioprinting of scaffold materials that will be overlaid with the patient's own cells, such as the pioneering work being done by Dr. Anthony Atala at Wake Forest Institute for Regenerative Medicine. There are a number of researchers now working to understand how to use patient-specific cells (which has the tremendous benefit of lowering the risk of rejection by the body) in an effort to change the way we do organ transplants today.
Craniomaxillofacial surgeons are another of the primary users of this technology. They are using models of the patient’s skull as a template for cranial reconstruction cuts in cases of craniosynostosis (i.e., repairing a newborn's misshapen skull, which is a relatively common occurrence), mirror image models for facial reconstruction, cutting guides for maxilla and mandibular reconstruction, pre-operative bending of plates for mandibular reconstruction, brain vessel models, as well as vascular flow models.
In the orthopedic context, surgeons are using 3D printed templating and pre-bending in defect reconstruction in acetabular revision (pelvis); printed guides for reverse shoulder arthroplasty; models for resection planning, and custom osteotomy templates. Some orthopedic surgeons now are working in-house and perhaps more often with third-party medical device manufacturers to produce custom implants as well as 3D printed surgical positioning, cutting and drill guides. One hospital has even been fabricating bespoke braces for scoliosis patients. There really is an extraordinary breadth of uses that doctors are continually finding for this custom-oriented technology.
Generally, surgeon's note that when they begin to understand the utility and relative simplicity of 3D printing, they begin to identify creative fixes for problems they routinely experience. For example, one group created a patient-specific immobilization system for taking an MRI. An important, but likely currently underutilized, use of 3D printed models is as a tool to facilitate patient and family informed consent. It is hard to imagine that the average patient or family member gets anywhere near as much information from looking at a 2D CT scan as from a patient-specific 3D model they can look at and even hold in their hands. While we are not close to the day that we can just print off a 3D model like we were downloading and printing a picture from our computer, there will no doubt be better patient understanding of the procedure they or a loved one faces when we eventually can.
The Medical 3D Printing Process
So, who is doing what with 3D printing in the hospital context? Since there was not a readily available list of participating institutions, I prepared a list of hospitals in North America that have 3D printing programs. Many of the best names in clinical care are on the list of 40 institutions. While I'm sure there are others, here is a sampling of who is involved.
I have included a more comprehensive list at the end of this article (based on what I could find from public news sources) which includes information on the types of 3D printer used by each program, the medical departments involved and the clinical applications described in news stories about the program.
Clinical Applications of 3D Printing in Surgery
So, how is 3D printing being used today? It spans the gamut from helping nearly 30 doctors and operating room personnel to visualize and communicate about the complex process of separating conjoined twins (as done in 2006 at the Mayo Clinic) to a more routine use as an orthopedic custom cutting guide for knee replacement surgery.
Cardiothoracic surgeons are now using 3D printed heart models with increasing frequency, particularly for pediatric cases. They use the models for pre-surgical planning, intraoperative visualization and even for training and technique practice using models printed with flexible, almost realistic material properties. Another use case involves planning and simulation of complex endovascular aortic repair. Surgeons use models to better plan for cases of Arteriovenus malformations (AVM) and cases involving ventricular septal defects (a hole in a wall of the heart). They are also using models to pre-plan and practice transcatheter valve positioning and for heart valve replacement planning. In a discussion of the use of 3D printing in cardiothoracic surgery, Dr. Stephen Cassivi of the Mayo Clinic described what he referred to as "the power of touch" and how these models can enhance the surgeon's understanding of complex or unusual anatomy. In fact, several surgeons mentioned the concept of "If I touch it, I own it."
A well publicized life-saving use of 3D printing technology involved the University of Michican CS Mott Children's Hospital's use of an implantable, bioresorbable splint for a young boy's tracheo-bronchomalacia (thinning of the wall(s) of the airway). The surgeons sought and received emergency approval from the FDA to use a 3D printed splint that used materials that would be resorbed into the patient's body over the course of several years but in the mean time would act as a scaffold on which the patient's own cells could regrow. This case is at the intersection of what I think of as the now of medical 3DP and its future. The future of medical 3DP is expected to involve the 3D bioprinting of scaffold materials that will be overlaid with the patient's own cells, such as the pioneering work being done by Dr. Anthony Atala at Wake Forest Institute for Regenerative Medicine. There are a number of researchers now working to understand how to use patient-specific cells (which has the tremendous benefit of lowering the risk of rejection by the body) in an effort to change the way we do organ transplants today.
Craniomaxillofacial surgeons are another of the primary users of this technology. They are using models of the patient’s skull as a template for cranial reconstruction cuts in cases of craniosynostosis (i.e., repairing a newborn's misshapen skull, which is a relatively common occurrence), mirror image models for facial reconstruction, cutting guides for maxilla and mandibular reconstruction, pre-operative bending of plates for mandibular reconstruction, brain vessel models, as well as vascular flow models.
In the orthopedic context, surgeons are using 3D printed templating and pre-bending in defect reconstruction in acetabular revision (pelvis); printed guides for reverse shoulder arthroplasty; models for resection planning, and custom osteotomy templates. Some orthopedic surgeons now are working in-house and perhaps more often with third-party medical device manufacturers to produce custom implants as well as 3D printed surgical positioning, cutting and drill guides. One hospital has even been fabricating bespoke braces for scoliosis patients. There really is an extraordinary breadth of uses that doctors are continually finding for this custom-oriented technology.
Generally, surgeon's note that when they begin to understand the utility and relative simplicity of 3D printing, they begin to identify creative fixes for problems they routinely experience. For example, one group created a patient-specific immobilization system for taking an MRI. An important, but likely currently underutilized, use of 3D printed models is as a tool to facilitate patient and family informed consent. It is hard to imagine that the average patient or family member gets anywhere near as much information from looking at a 2D CT scan as from a patient-specific 3D model they can look at and even hold in their hands. While we are not close to the day that we can just print off a 3D model like we were downloading and printing a picture from our computer, there will no doubt be better patient understanding of the procedure they or a loved one faces when we eventually can.
The Medical 3D Printing Process
Credit: I produced this graphic using images from Siemens, Materialise and 3D Systems
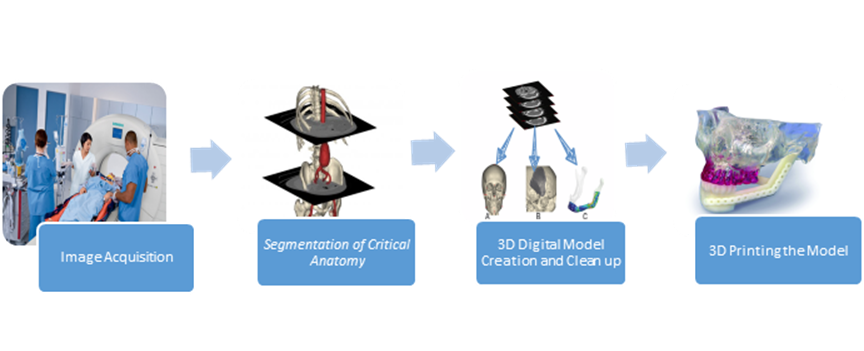
The medical image to STL workflow
The process of creating a patient-specific 3D printed model of relevant anatomy starts with the 2D technology that surgeons have been using for decades. Image acquisition can be conducted via Computed Tomography (CT), Magnetic Resonance (MR), Echocardiography, PET scan or other modalities. As you might imagine, it is keenly important that a good image is acquired as that forms the basis of the eventual model. Close coordination between the radiologist and the surgeon is critical as it enables the doctors and/or technicians who are acquiring the medical image to take into account exactly what the surgeon wants to see and the planned use of the model.
After a good image is acquired, segmentation involves focusing only on the relevant anatomic structures and removing unnecessary elements from the medical image (say, skin, tissue, blood vessels, and organs not related to the surgery). This step is the most resource intensive element of the work flow and can take anywhere from 1 to 15 hours of a skilled technician or radiologist's time depending on the complexity of the segmentation output desired, the quality of the image, the existence of artifacts in the image (e.g., when a patient already has metal in their body), and other factors. Segmentation can involve the use of color coded anatomy to facilitate visual differentiation of anatomical structures or even pathologies such as tumors. The segmentation process (and follow-on step) is achieved using one of several software programs such as Materialise's MIMICS Innovation Suite, Vital Images, Inc's Vitrea both of which are 510(k) cleared by the FDA or potentially via an open source software like Osirix or 3D Slicer.
3D digital model creation involves accurately converting the 2D medical image data to a 3D digital model. Since the typical CT scans range from sub-millimeter slices to up to 5 mm, there will be some extrapolation between images. That is another reason that good communication between surgeon and radiologist is important as what density of images is required will depend on what level of information the model will need to provide.
Finally, printing the 3D model can be accomplished on a variety of machines which can print in multiple materials and colors. There are literally hundreds of 3D printers on the market at this point. The main considerations (which can quickly cut through many of the machines on the market) are 1) the intended use of the model (e.g., for planning, visualization, as a surgical instrument, technique practice, implant or other), whether one or more colors are needed for the model, the desired material properties (e.g, metal, many types of plastic including flexible materials, or other properties), sterilization requirements, size of the model, and, of course, budget.
Key Benefits of the Technology
The benefits reported by surgeons who are currently using 3D printing in their medical practice are as follows:
At this point, only some of these benefits have begun to be quantified. Most are mainly the anecdotal (yet earnest) findings of surgeons involved in the practice. Over time, as discussed below, it is expected that clinical trials and other science-based methodologies will be employed to document and quantify these benefits. It is also too early to tell the economic impact of 3D printing in hospitals, but as some doctors have suggested, at upwards of $4,000 per hour for OR time, it is not that hard to envision how there could be a reasonable return on investment based on reduced OR time alone and independent of any other benefits.
Current Challenges Being Addressed
Lack of reimbursement Any new surgical technology is going to be viewed through the lens of its cost effectiveness and how it can be paid for. The case for reimbursement generally begins with data. Insurers not only want to see data that a new technology or therapy meets the minimum criteria of clinical efficacy and safety but also now want to know that the new technology or therapy improves the clinical outcomes of patients compared with existing approaches.
Since facilitating better outcomes should be the primary measure of a new technology's utility, it is appropriate to ask what scientific, reproducible clinical data is out there to bolster the claim that 3D printing improves patient outcomes. That data is starting to be collected and compiled to add to the substantial experiential and anecdotal evidence. An exciting effort on that front is a clinical trial involving Phoenix Children’s Hospital, Children’s Hospital of Philadelphia, and Children’s National Medical Center. This trial represents the first attempt at describing the statistically significant benefits of planning surgeries based on 3D printed models. The trial will include nearly 200 patient cases to study statistical significance in surgical outcomes including surgical time, duration of hospital stay, and 30-day mortality. Assuming that the surgeons' current hypotheses are confirmed with respect to the benefits of 3DP, this is precisely the type of clinical evidence that can accelerate adoption of 3DP as an effective modality as well as start to make the case for cost-reimbursement. While there will no doubt be additional disease state and surgical procedure-specific clinical trials, there may also need to be meta analyses where possible to explore whether the benefits of 3D printing in a single type of surgery can be extrapolated more broadly.
Lack of information on how to get started One of the greatest challenges to making the use of this technology ubiquitous, which expert surgeons believe is both important and inevitable, is knowing how to set up a program properly. Establishing a 3D printing program in a hospital is an investment and the usual business case of procedure-based reimbursement does not yet apply. The best guess of experts was somewhere between three and five years for reimbursement. Therefore pre-reimbursement, there will be a different calculation for the hospital administrator deciding whether to start up a program.
One of the challenges that hospitals thinking about instituting a 3D printing program have is the paucity of information out there about starting a program. It became clear to me from talking to attendees that implementation guidance would be useful and is now in demand. Reaching out for some basic consulting services is a good idea for hospitals thinking of building out a program because this is an investment, one which requires pre-planning and prudence to be done wisely.
In talking with a number of the people at the recent Mayo event, I learned that there is significant demand by hospitals for the type of information discussed at the event as well as basic support in thinking through the considerations necessary before starting a hospital-based program. I have spoken with a number of people who said that their institutions had purchased 3D printers first before figuring out what they were going to do with them or who was going to do what as a part of the 3D printing program. It won't always be, but that could be a recipe for an expensive 3D printer gathering dust in a corner of the hospital.
In talking with the Mayo Clinic's head of Radiology (a group of 180 radiologists!) Dr. Kent Thielen, I learned that hospitals around the country regularly call him and his team in an effort to come up to speed on the issues around 3D printing in hospitals. This is very time-consuming for the experts at Mayo but they have generously done this work in order to help their colleagues at other institutions. However, Dr. Thielen indicated that they have had to throttle back some of that consultative help simply due to the sheer volume of requests.
I went to the conference to understand whether there was demand for program implementation consulting services and whether the technology is ready for wider spread adoption in the near term. I believe the answer to both of those questions is yes.
So, where can interested hospital teams learn about the process of implementing a 3D printing program in their hospitals? There are currently a few places to learn and I expect there to be others available in the future.
There is now a great web-based resource on using 3D printing in healthcare applications. The website 3dadvantage.org was established by David Escobar, CHSOS and EMT, who works as a Simulation Specialist at Cedars-Sinai Medical Center in Los Angeles. David is a pioneer in this space and his website and blog is a good resource for people wanting to learn about 3D printing in the hospital context. David and the Cedars-Sinai team has built a 3D printing program and he is now teaching others about what they have learned about the process, the technology and how to make it work.
Another good resource is 3D Heals.com. Referring to itself as a healthcare 3D printing innovation platform, the site offers those interested in 3D printing in the healthcare context educational resources, data regarding the global impact of 3D printing and bioprinting technologies, as well as a way to meet up with others who are already involved in using the technology.
At the Mayo Clinic event Jane M. Matsumoto, M.D. and Jonathan M. Morris, M.D. indicated that a society dedicated to promoting 3D printing in medical practice is in the works. That of course would be a tremendous step forward for adoption of this important technology.
All of these efforts seem like just what is needed at this point in the technology adoption curve. The initial groundwork has been laid by the pioneering surgeons who have shown and now are routinely continuing to underscore the utility of 3D printing as a key new innovation that can improve surgical outcomes. The earliest adopters have shown that this technology is feasible and flexible. We are now experiencing the next round of early adopters who are taking what has been learned and demonstrated and expanding it to new areas of utility. As these new uses become more common, and in some cases the new standard of care, additional hospitals and surgeons are going to need to become educated on how to use this new tool. Some of that will happen in medical schools, but much of that learning will need to take place in hospitals around the country and at terrific learning opportunities like the Mayo Clinic's and RSNA events.
Starting up a hospital-based 3D printing program
There are a number of practical considerations that need to be thought through before undertaking a 3D printing program in the hospital. The initial question should be does the hospital have the appropriate personnel resources (with the right skill sets and level of interest) for such a program? For example, the hardest part of taking a medical image and turning it into something useful for the surgeon is the segmentation process. As part of that work flow, someone with a detailed knowledge of human anatomy must segment (separate) the critical anatomy that is important to the surgeon from all the other images and visual artifacts that come out of the CT or MRI. Is that something the hospital is ready to take on?
There are a number of other pre-investment decisions that need to be made in order to be strategic about how to use 3D printing in your hospital. For example, there are personnel and space considerations, hardware and software options, medical protocols and workflow decisions. Each of these should be considered before purchasing a 3D printer. And on the decision of what type of 3D printer to buy, many surgeons using 3D printing today advise that the type of printer is not the first decision, but rather a pretty straight-forward final decision, once the programs' objectives have been determined. It is worth noting that, depending on the types of cases that are handled in the hospital, a program might be able to start up a program with an inexpensive $3,500 printer and part-time skilled technician overseen by a radiologist rather than a more robust program with dedicated technicians, supporting biomedical engineers and/or physicists, a dedicated lab and a $400,000 printer. There are a wide range of appropriate options, including even outsourcing some or all of the segmentation and 3D printing work to third parties. Establishing a well-planned 3D printing program requires going over the available options and picking a strategy that fits the hospital's needs.
Future Expansion of the Use of 3DP in Medical Practice
There are at least four ways the adoption of 3D printing will spread throughout hospitals in North America. The first is the approach that is currently being pursued. That involves hospital administrators and surgeons who are interested in adopting a 3D printing program calling the experts at Mayo Clinic (and increasingly colleagues at other institutions) and asking them how they did it. As you might guess that is fairly time-consuming for the experts who have patients of their own to care for. While they have been helping other hospitals today out of a sense of collegiality and a desire to see this technology spread, there are only so many hours in the day for them to provide such services.
The second way that 3DP in the hospital can expand its adoption is for an advocate in a hospital to simply try it and take an experimental approach by buying a 3D printer and software to get a feel for how it works, reading the relevant literature, attending relevant conferences and talking to others who have done it. There will no doubt be a certain amount of this, but this may not be the most efficient way to introduce an important new surgical technique into North American hospitals.
The Third way will include one or more groups of people providing implementation guidance (consulting services) to hospitals who are considering starting a program. That will have the benefit of freeing up some of the Mayo Clinic's and other experts' time and would act as a force multiplier by covering the basic considerations of who, what, when, how and how much when considering establishing a new program and leaving time for the more complex discussions of clinical applications to the doctors. I will mention that my company, Visuality LLC is now providing implementation guidance services to hospitals considering a 3D printing program. I see 3D printing in the hospital context as an incredibly powerful tool for clinicians and I want to help hospitals make good choices as they bring this technology online.
The fourth means of adoption involves teaching about these techniques in medical school and having the new generation of surgeons learn about the use of 3D printing as part of their medical education. That will happen and the hospitals where they go to practice will then start to feel some pressure to bring those technologies to use in their hospitals, perhaps even as a means of attracting the top surgical talent.
So where will hospital based 3D printing go from here?
What is clear is that 3D printing in the hospital context is a useful tool for surgeons. That utility will drive the practice's adoption in an increasing number of hospitals. With its broad range of uses, there is no reason to suspect that it won't ultimately be used in all hospitals in some variation or other depending on the types of patients and surgical cases handled by the hospital.
I expect the software involved in the segmentation process to continue to improve and to some extent even begin to automate the segmentation process. Some level of automated segmentation could greatly speed up the process, which is currently the long pole in the tent.
The next truly exciting area of 3D printing after use as anatomical models, surgical aids and the current range of titanium and other implants is for bio printing and regenerative medicine. I briefly discussed the work of Dr. Atala above and this area of research holds the very real promise of changing the way we conduct transplant surgery. With bioprinted scaffolds in the shape of a patient's organ and using the patient's own cells, we may ultimately be able to create transplantable organs that preclude the need for donors.
The medical image to STL workflow
The process of creating a patient-specific 3D printed model of relevant anatomy starts with the 2D technology that surgeons have been using for decades. Image acquisition can be conducted via Computed Tomography (CT), Magnetic Resonance (MR), Echocardiography, PET scan or other modalities. As you might imagine, it is keenly important that a good image is acquired as that forms the basis of the eventual model. Close coordination between the radiologist and the surgeon is critical as it enables the doctors and/or technicians who are acquiring the medical image to take into account exactly what the surgeon wants to see and the planned use of the model.
After a good image is acquired, segmentation involves focusing only on the relevant anatomic structures and removing unnecessary elements from the medical image (say, skin, tissue, blood vessels, and organs not related to the surgery). This step is the most resource intensive element of the work flow and can take anywhere from 1 to 15 hours of a skilled technician or radiologist's time depending on the complexity of the segmentation output desired, the quality of the image, the existence of artifacts in the image (e.g., when a patient already has metal in their body), and other factors. Segmentation can involve the use of color coded anatomy to facilitate visual differentiation of anatomical structures or even pathologies such as tumors. The segmentation process (and follow-on step) is achieved using one of several software programs such as Materialise's MIMICS Innovation Suite, Vital Images, Inc's Vitrea both of which are 510(k) cleared by the FDA or potentially via an open source software like Osirix or 3D Slicer.
3D digital model creation involves accurately converting the 2D medical image data to a 3D digital model. Since the typical CT scans range from sub-millimeter slices to up to 5 mm, there will be some extrapolation between images. That is another reason that good communication between surgeon and radiologist is important as what density of images is required will depend on what level of information the model will need to provide.
Finally, printing the 3D model can be accomplished on a variety of machines which can print in multiple materials and colors. There are literally hundreds of 3D printers on the market at this point. The main considerations (which can quickly cut through many of the machines on the market) are 1) the intended use of the model (e.g., for planning, visualization, as a surgical instrument, technique practice, implant or other), whether one or more colors are needed for the model, the desired material properties (e.g, metal, many types of plastic including flexible materials, or other properties), sterilization requirements, size of the model, and, of course, budget.
Key Benefits of the Technology
The benefits reported by surgeons who are currently using 3D printing in their medical practice are as follows:
- The technology shortens surgical procedure time
- Improves communication and collaboration between and among different members of the surgical team, including surgeons and other operating room staff
- Enhances pre-operative planning and enables a better tactile understanding of unique anatomy
- Models can be used as a reference during surgery (replacing awkward computer-based options)
- Patient-specific surgical guides minimize freehand error risk
- Mirror-image modeling used for reconstruction templating facilitates a more natural outcome for the patient
- Good for overcoming the challenge of restricted resident work hours by permitting them to practice on models (whereas they formerly got more surgical reps)
- Surgeons can customize off-the shelf devices pre-operatively to fit patient's anatomy
- Helps move certain surgeries from procedures with variable outcomes requiring more intuition toward procedures that are routine, guided, reproducible with similar outcomes each time
- More effective education of patients, improves informed consent
- Better patient outcomes (morbidity, mortality and recuperation time)
At this point, only some of these benefits have begun to be quantified. Most are mainly the anecdotal (yet earnest) findings of surgeons involved in the practice. Over time, as discussed below, it is expected that clinical trials and other science-based methodologies will be employed to document and quantify these benefits. It is also too early to tell the economic impact of 3D printing in hospitals, but as some doctors have suggested, at upwards of $4,000 per hour for OR time, it is not that hard to envision how there could be a reasonable return on investment based on reduced OR time alone and independent of any other benefits.
Current Challenges Being Addressed
Lack of reimbursement Any new surgical technology is going to be viewed through the lens of its cost effectiveness and how it can be paid for. The case for reimbursement generally begins with data. Insurers not only want to see data that a new technology or therapy meets the minimum criteria of clinical efficacy and safety but also now want to know that the new technology or therapy improves the clinical outcomes of patients compared with existing approaches.
Since facilitating better outcomes should be the primary measure of a new technology's utility, it is appropriate to ask what scientific, reproducible clinical data is out there to bolster the claim that 3D printing improves patient outcomes. That data is starting to be collected and compiled to add to the substantial experiential and anecdotal evidence. An exciting effort on that front is a clinical trial involving Phoenix Children’s Hospital, Children’s Hospital of Philadelphia, and Children’s National Medical Center. This trial represents the first attempt at describing the statistically significant benefits of planning surgeries based on 3D printed models. The trial will include nearly 200 patient cases to study statistical significance in surgical outcomes including surgical time, duration of hospital stay, and 30-day mortality. Assuming that the surgeons' current hypotheses are confirmed with respect to the benefits of 3DP, this is precisely the type of clinical evidence that can accelerate adoption of 3DP as an effective modality as well as start to make the case for cost-reimbursement. While there will no doubt be additional disease state and surgical procedure-specific clinical trials, there may also need to be meta analyses where possible to explore whether the benefits of 3D printing in a single type of surgery can be extrapolated more broadly.
Lack of information on how to get started One of the greatest challenges to making the use of this technology ubiquitous, which expert surgeons believe is both important and inevitable, is knowing how to set up a program properly. Establishing a 3D printing program in a hospital is an investment and the usual business case of procedure-based reimbursement does not yet apply. The best guess of experts was somewhere between three and five years for reimbursement. Therefore pre-reimbursement, there will be a different calculation for the hospital administrator deciding whether to start up a program.
One of the challenges that hospitals thinking about instituting a 3D printing program have is the paucity of information out there about starting a program. It became clear to me from talking to attendees that implementation guidance would be useful and is now in demand. Reaching out for some basic consulting services is a good idea for hospitals thinking of building out a program because this is an investment, one which requires pre-planning and prudence to be done wisely.
In talking with a number of the people at the recent Mayo event, I learned that there is significant demand by hospitals for the type of information discussed at the event as well as basic support in thinking through the considerations necessary before starting a hospital-based program. I have spoken with a number of people who said that their institutions had purchased 3D printers first before figuring out what they were going to do with them or who was going to do what as a part of the 3D printing program. It won't always be, but that could be a recipe for an expensive 3D printer gathering dust in a corner of the hospital.
In talking with the Mayo Clinic's head of Radiology (a group of 180 radiologists!) Dr. Kent Thielen, I learned that hospitals around the country regularly call him and his team in an effort to come up to speed on the issues around 3D printing in hospitals. This is very time-consuming for the experts at Mayo but they have generously done this work in order to help their colleagues at other institutions. However, Dr. Thielen indicated that they have had to throttle back some of that consultative help simply due to the sheer volume of requests.
I went to the conference to understand whether there was demand for program implementation consulting services and whether the technology is ready for wider spread adoption in the near term. I believe the answer to both of those questions is yes.
So, where can interested hospital teams learn about the process of implementing a 3D printing program in their hospitals? There are currently a few places to learn and I expect there to be others available in the future.
There is now a great web-based resource on using 3D printing in healthcare applications. The website 3dadvantage.org was established by David Escobar, CHSOS and EMT, who works as a Simulation Specialist at Cedars-Sinai Medical Center in Los Angeles. David is a pioneer in this space and his website and blog is a good resource for people wanting to learn about 3D printing in the hospital context. David and the Cedars-Sinai team has built a 3D printing program and he is now teaching others about what they have learned about the process, the technology and how to make it work.
Another good resource is 3D Heals.com. Referring to itself as a healthcare 3D printing innovation platform, the site offers those interested in 3D printing in the healthcare context educational resources, data regarding the global impact of 3D printing and bioprinting technologies, as well as a way to meet up with others who are already involved in using the technology.
At the Mayo Clinic event Jane M. Matsumoto, M.D. and Jonathan M. Morris, M.D. indicated that a society dedicated to promoting 3D printing in medical practice is in the works. That of course would be a tremendous step forward for adoption of this important technology.
All of these efforts seem like just what is needed at this point in the technology adoption curve. The initial groundwork has been laid by the pioneering surgeons who have shown and now are routinely continuing to underscore the utility of 3D printing as a key new innovation that can improve surgical outcomes. The earliest adopters have shown that this technology is feasible and flexible. We are now experiencing the next round of early adopters who are taking what has been learned and demonstrated and expanding it to new areas of utility. As these new uses become more common, and in some cases the new standard of care, additional hospitals and surgeons are going to need to become educated on how to use this new tool. Some of that will happen in medical schools, but much of that learning will need to take place in hospitals around the country and at terrific learning opportunities like the Mayo Clinic's and RSNA events.
Starting up a hospital-based 3D printing program
There are a number of practical considerations that need to be thought through before undertaking a 3D printing program in the hospital. The initial question should be does the hospital have the appropriate personnel resources (with the right skill sets and level of interest) for such a program? For example, the hardest part of taking a medical image and turning it into something useful for the surgeon is the segmentation process. As part of that work flow, someone with a detailed knowledge of human anatomy must segment (separate) the critical anatomy that is important to the surgeon from all the other images and visual artifacts that come out of the CT or MRI. Is that something the hospital is ready to take on?
There are a number of other pre-investment decisions that need to be made in order to be strategic about how to use 3D printing in your hospital. For example, there are personnel and space considerations, hardware and software options, medical protocols and workflow decisions. Each of these should be considered before purchasing a 3D printer. And on the decision of what type of 3D printer to buy, many surgeons using 3D printing today advise that the type of printer is not the first decision, but rather a pretty straight-forward final decision, once the programs' objectives have been determined. It is worth noting that, depending on the types of cases that are handled in the hospital, a program might be able to start up a program with an inexpensive $3,500 printer and part-time skilled technician overseen by a radiologist rather than a more robust program with dedicated technicians, supporting biomedical engineers and/or physicists, a dedicated lab and a $400,000 printer. There are a wide range of appropriate options, including even outsourcing some or all of the segmentation and 3D printing work to third parties. Establishing a well-planned 3D printing program requires going over the available options and picking a strategy that fits the hospital's needs.
Future Expansion of the Use of 3DP in Medical Practice
There are at least four ways the adoption of 3D printing will spread throughout hospitals in North America. The first is the approach that is currently being pursued. That involves hospital administrators and surgeons who are interested in adopting a 3D printing program calling the experts at Mayo Clinic (and increasingly colleagues at other institutions) and asking them how they did it. As you might guess that is fairly time-consuming for the experts who have patients of their own to care for. While they have been helping other hospitals today out of a sense of collegiality and a desire to see this technology spread, there are only so many hours in the day for them to provide such services.
The second way that 3DP in the hospital can expand its adoption is for an advocate in a hospital to simply try it and take an experimental approach by buying a 3D printer and software to get a feel for how it works, reading the relevant literature, attending relevant conferences and talking to others who have done it. There will no doubt be a certain amount of this, but this may not be the most efficient way to introduce an important new surgical technique into North American hospitals.
The Third way will include one or more groups of people providing implementation guidance (consulting services) to hospitals who are considering starting a program. That will have the benefit of freeing up some of the Mayo Clinic's and other experts' time and would act as a force multiplier by covering the basic considerations of who, what, when, how and how much when considering establishing a new program and leaving time for the more complex discussions of clinical applications to the doctors. I will mention that my company, Visuality LLC is now providing implementation guidance services to hospitals considering a 3D printing program. I see 3D printing in the hospital context as an incredibly powerful tool for clinicians and I want to help hospitals make good choices as they bring this technology online.
The fourth means of adoption involves teaching about these techniques in medical school and having the new generation of surgeons learn about the use of 3D printing as part of their medical education. That will happen and the hospitals where they go to practice will then start to feel some pressure to bring those technologies to use in their hospitals, perhaps even as a means of attracting the top surgical talent.
So where will hospital based 3D printing go from here?
What is clear is that 3D printing in the hospital context is a useful tool for surgeons. That utility will drive the practice's adoption in an increasing number of hospitals. With its broad range of uses, there is no reason to suspect that it won't ultimately be used in all hospitals in some variation or other depending on the types of patients and surgical cases handled by the hospital.
I expect the software involved in the segmentation process to continue to improve and to some extent even begin to automate the segmentation process. Some level of automated segmentation could greatly speed up the process, which is currently the long pole in the tent.
The next truly exciting area of 3D printing after use as anatomical models, surgical aids and the current range of titanium and other implants is for bio printing and regenerative medicine. I briefly discussed the work of Dr. Atala above and this area of research holds the very real promise of changing the way we conduct transplant surgery. With bioprinted scaffolds in the shape of a patient's organ and using the patient's own cells, we may ultimately be able to create transplantable organs that preclude the need for donors.
Conclusion
The reality is that medicine, and particularly surgery, fundamentally requires disciplined scientists who are also skilled artists and artisans and the best surgeons appear to be a creative mix of all three. Surgical technique isn't static but rather changes, develops and improves over time. The true value of 3D printing is that it gives the surgeon one more flexible tool for making surgeries lower risk, swifter and ultimately more effective.
From the exotic to the mundane, 3D printing in the medical context is both here to stay and will rapidly grow over the next several years culminating in an explosion of adoption when reimbursable. The best part of this trending phenomenon to me is that it uses 3D printing's unique ability to customize patient-specific solutions in a very practical way and that it has so much ability to improve patient care and even save lives. I believe that this is one of the very best uses of 3D printing technology in practice today.
To learn more about how Visuality LLC can help your hospital as it considers using 3D printing technology, feel free to contact me at jonathan.c.ritter@gmail.com or 908.745.9751. Now is an excellent time to get started using 3DP technology. I would be happy to answer your questions and help your institution use its resources wisely as your program begins. I am available to speak with doctors and/or administrators who want to learn more about the 3D printing process and how it might be used in their hospital. I am pleased to offer a complimentary overview presentation for interested hospitals. After that, for those institutions who are thinking about moving forward, I am available for a reasonable fee to help administrators identify the key questions they should be asking and think through the options available before making any significant investment in program resources.
The reality is that medicine, and particularly surgery, fundamentally requires disciplined scientists who are also skilled artists and artisans and the best surgeons appear to be a creative mix of all three. Surgical technique isn't static but rather changes, develops and improves over time. The true value of 3D printing is that it gives the surgeon one more flexible tool for making surgeries lower risk, swifter and ultimately more effective.
From the exotic to the mundane, 3D printing in the medical context is both here to stay and will rapidly grow over the next several years culminating in an explosion of adoption when reimbursable. The best part of this trending phenomenon to me is that it uses 3D printing's unique ability to customize patient-specific solutions in a very practical way and that it has so much ability to improve patient care and even save lives. I believe that this is one of the very best uses of 3D printing technology in practice today.
To learn more about how Visuality LLC can help your hospital as it considers using 3D printing technology, feel free to contact me at jonathan.c.ritter@gmail.com or 908.745.9751. Now is an excellent time to get started using 3DP technology. I would be happy to answer your questions and help your institution use its resources wisely as your program begins. I am available to speak with doctors and/or administrators who want to learn more about the 3D printing process and how it might be used in their hospital. I am pleased to offer a complimentary overview presentation for interested hospitals. After that, for those institutions who are thinking about moving forward, I am available for a reasonable fee to help administrators identify the key questions they should be asking and think through the options available before making any significant investment in program resources.
3D Printing in Hospitals in North America
Note: The following list is intended to begin the process of compiling a list of institutions employing 3D printing in the hospital context. It was created in March 2016 based on news reports, hospital websites and other public sources and so is likely to contain some outdated or incomplete information. This list is intended to serve as the kernel for a comprehensive list of programs nationwide. I am hopeful that this list can be helpful in facilitating the type of collaboration among institutions that the speakers at the CME conference said was essential to the expanded use of 3D printing nation-wide. The list will no doubt benefit from input directly from the institutions to ensure that it is accurate and up-to-date. Please feel free to copy, add to, share, update and improve this list.
I have broken out each entry to include:
Name of Institution
Location
Departments Involved
Clinical Applications
Printer Hardware
Boston Children's Hospital
Massachusetts, Boston
Neurosurgery, Cerebrovascular Surgery, Craniofacial Surgery, Radiology
Arteriovenus malformation (AVM) models, pediatric device discovery and prototyping, pre-surgical planning, models of patient’s skull for craniosynostosis, spines, rib cages and blood vessels
Stratasys Connex500
Brigham and Women's Hospital
Massachusetts, Boston
Plastic Surgery, Urology, Cardiac Surgery, Radiology Thoracic Surgery, biomedical engineering
facial transplants, bio-printing blood vessels
Stratasys Objet500 Connex3; Objet Eden 260VS; bioprinter
Cedars-Sinai Medical Center
California, Los Angeles
Cardiac Surgery
Heart models
Makerbot Replicator 2 and 2X, Formlabs Form1+, CubePro Duo
Children's Hospital of Illinois
Illinois, Peoria
Pediatric Cardiology
Pediatric heart models and training aids
3D Systems ZPrinter 450
Children’s Hospital of Oakland
California, Oakland
Pediatric Orthopedic Surgery
Bespoke braces for scoliosis
Unknown
Children’s Hospital of Philadelphia
Pennsylvania, Philadelphia
Cardiac Surgery
Heart models,
Stratasys Objet500 Connex
Cincinnati Children's Hospital
Ohio, Cincinnati
Cardiac, Pediatric plastic surgery
Heart models, birthmark removal via tissue expanders
Makerbot Replicator Z18
Denver University
Colorado, Denver
Cardiac Biomechanics Lab
heart models, bio printing research on artificial heart valves
BioBot 1
Erlanger
Medical Center
Tennessee, Chattanooga
Urology and other departments
Heart models, kidney tumor for patient education
Outsourcing 3D printing to Chattanooga based 3D Ops which uses the Stratasys Connex and other printers
Feinberg School of Medicine at Northwestern University
Illinois, Chicago
Pediatric Orthopedics, Radiology and General Surgery
Pediatric orthopedics and general surgical training
Unknown
Henry Ford Hospital
Michigan, Detroit
Cardiothoracic Surgery, Innovation Institute, Radiology
Heart models, transcatheter valve positioning, heart valve replacement planning
Unknown
Hospital for Sick Children
Ontario, Toronto
Pediatric Cardiology
Heart models for complex surgical training and patient education
Objet260 Connex
Houston Methodist
Texas, Houston
Neurosurgery, Cardiac Surgery, HM Research Institute
Heart models, bio printing research
MakerBot Replicator 2 and others
Jacobs Institute
New York, Buffalo
Neurosurgery, Biomedical Engineering
Brain vessel models, Vascular flow models
Stratasys Eden 260V
Kosair Children's Hospital
Kentucky, Louisville
Pediatric Cardiac Surgery
Heart models
Makerbot Replicator 2X
Lehigh Valley Health Network
Exploratory study
Not clear from reports whether program moved forward
Mayo Clinic
Minnesota, Rochester
Cardiac Surgery, General Surgery, Neurosurgery, Oncology, Oral and Maxillofacial Surgery, Orthopedic Surgery, Otorhinolaryngology, Pediatric Surgery, Plastic and Reconstructive Surgery, Radiology, Thoracic Surgery, Transplant Center, Urology, Vascular and Endovascular Surgery
Heart models, kidney models for renal sparing surgery, planning and simulation of complex endovascular aortic repair, patient-specific immobilization system for MRI, pre-operative bending for mandibular reconstruction, mirror image models for facial reconstruction, cutting guides for maxilla and mandibular reconstruction, templating and pre-bending in defect reconstruction in acetabular revision, guides for reverse shoulder arthroplasty, intraoperative localization and templating for orthopedic surgery, resection planning, custom osteotomy template,
Stratasys Connex 350 polyjet
Montefiore Medical Center, [University Hospital for Albert Einstein College of Medicine]
New York City
Pediatric Neurosurgery, Pediatric Rehabilitation, Craniofacial Surgery, Radiology, Plastic and Reconstructive Surgery
Cranial reconstruction for Craniosynostosis, Upper extremity prosthesis
Outsources cosmetic surgery models to Mirror Me 3D
Mount Sinai Hospital
Ontario, Toronto
Pathology, Institute of Biomaterials and Biomedical Engineering
Joint replacement
Unknown
Nemours / Alfred I. DuPont Hospital for Children
Delaware, Wilmington
Orthopedic Surgery
Pediatric prostheses
Stratasys Dimension 3D printer
New York- Presbyterian Morgan Stanley Children’s Hospital
New York City
Pediatric Cardiology
Pediatric heart models
Have outsourced printing to Materialise in past. Moved in-house?
Niklaus Children's Hospital
Florida, Miami
Pediatric Cardiology
Pediatric heart models
Stratasys Connex3
Phoenix Children's Hospital
Phoenix Arizona
Neurosurgery, Oncology, Cardiac
Heart models, brain tumors for “patient empowerment”
3D Systems ZCorp 650 and 3 others for different materials
Rady Children's hospital
California, San Diego
Pediatric Cardiac Surgery
heart models for planning complex heart surgeries and family education
Rady is outsourcing the printing of models to local providers.
Seattle Children's Hospital
Washington, Seattle
Cardiac Surgery, Oral and maxillofacial Surgery, Neurosurgery, Radiology
Heart models, cranium models
HeartMAP™ Simulator
Shriner’s Hospital for
Children
Texas, Houston
Orthopedic Surgery, Bioengineering students from Rice
prosthetic hands
Unknown
Shriners Hospital for Children
Illinois, Chicago
Craniomaxillofacial Surgery, Radiology, Pediatric Spine Surgery
Craniofacial reconstructions, cranial vault implant, cutting guides and templates, Spine models
Printing outsourced to the Jump Trading Simulation and Education Institute and Medical Modeling Inc.
Stanford Medical Center
[Note: This entry needs work; sources are less definitive than usual. Since Stanford is my alma mater, I hate to do it an injustice!]
California, Palo Alto
Orthopedic Surgery, Craniomaxillofacial Surgery
Pre-operative plate bending template, research on polymer-, ceramic-, hydrogel-based, and hybrid scaffolds with well-defined complex geometry and highly-reproducible controlled porous architecture.
3D Systems Projet and in-house fabrication system
St. Louis Children’s Hospital
Missouri, St. Louis
Cardiology
Heart models
3D Systems
University of Colorado School of Medicine
Colorado, Denver
Biomedical Lab
Metal parts for prosthetics
Germany-based EOS direct metal laser sintering printer.
University of Illinois College of Medicine
Illinois, Peoria
Craniofacial, Cardiac Surgery
Heart models
Printing outsourced to the Jump Trading Simulation and Education Institute
University of Michigan CS Mott Children’s Hospital
Michigan, Ann Arbor
Pediatric Surgery, Pediatric Otolaryngology, Biomedical Engineering
Implantable bioresorbable splint for tracheo-bronchomalacia, assessment of need for Ex Utero Intrapartum Treatment (EXIT) Procedure, 3D biomaterial printing
EOS Formiga P100 selective laser sintering building the splints with a polycaprolactone material (biodegradable polymer).
University of Pennsylvania Medical Center
Pennsylvania, Philadelphia
Maxillofacial, Orthopedic
Orthopedic implants
Unknown
University of Ottawa Hospital
[Need update from Frank Rybicki, MD]
Unknown
University of Toronto, Sunnybrook Health Sciences Centre
Ontario, Toronto
Plastic Surgery
skin bio printing for burn treatment
First gen prototype bio printer
University of Utah Health Sciences Center
Utah, Salt Lake City
Oncology
Prosthetic ear
Unknown
Wake Forest School of Medicine
North Carolina, Winston-Salem
Urology
Bio-printing of skin for burn treatment, research on printing of tissues and organs, regenerative medicine
Bespoke integrated tissue-organ printer (ITOP) which combines and layers hydrogels, human cells and biodegradable materials for structure.
Walter Reed National Military Medical Center, Medical Applications Center
Maryland, Bethesda
Craniofacial, Orthopedic, Dental, Radiology
Medical models, custom implants, surgical positioning, cutting and drill guides
3D Systems’ ZCorp 650 and 450, Arcam Electron Beam Melting (EBM), 3DS’ SLA 7000 and SLA 500, Viper Pro, Stratasys’ uPrint
Washington University School of Medicine
Missouri, St. Louis
Cardiothoracic Surgery, Otolaryngology
Heart models, prosthetic forearms and hands
Five printers including a BioBot.
Weill Cornell Medical College
New York City
Cardiothoracic Surgery
Research on bio-printing of heart valves, intervertebral disk repair
Makerbot Replicator 2, Stratasys uPrint and Fortus 250mc
Note: The following list is intended to begin the process of compiling a list of institutions employing 3D printing in the hospital context. It was created in March 2016 based on news reports, hospital websites and other public sources and so is likely to contain some outdated or incomplete information. This list is intended to serve as the kernel for a comprehensive list of programs nationwide. I am hopeful that this list can be helpful in facilitating the type of collaboration among institutions that the speakers at the CME conference said was essential to the expanded use of 3D printing nation-wide. The list will no doubt benefit from input directly from the institutions to ensure that it is accurate and up-to-date. Please feel free to copy, add to, share, update and improve this list.
I have broken out each entry to include:
Name of Institution
Location
Departments Involved
Clinical Applications
Printer Hardware
Boston Children's Hospital
Massachusetts, Boston
Neurosurgery, Cerebrovascular Surgery, Craniofacial Surgery, Radiology
Arteriovenus malformation (AVM) models, pediatric device discovery and prototyping, pre-surgical planning, models of patient’s skull for craniosynostosis, spines, rib cages and blood vessels
Stratasys Connex500
Brigham and Women's Hospital
Massachusetts, Boston
Plastic Surgery, Urology, Cardiac Surgery, Radiology Thoracic Surgery, biomedical engineering
facial transplants, bio-printing blood vessels
Stratasys Objet500 Connex3; Objet Eden 260VS; bioprinter
Cedars-Sinai Medical Center
California, Los Angeles
Cardiac Surgery
Heart models
Makerbot Replicator 2 and 2X, Formlabs Form1+, CubePro Duo
Children's Hospital of Illinois
Illinois, Peoria
Pediatric Cardiology
Pediatric heart models and training aids
3D Systems ZPrinter 450
Children’s Hospital of Oakland
California, Oakland
Pediatric Orthopedic Surgery
Bespoke braces for scoliosis
Unknown
Children’s Hospital of Philadelphia
Pennsylvania, Philadelphia
Cardiac Surgery
Heart models,
Stratasys Objet500 Connex
Cincinnati Children's Hospital
Ohio, Cincinnati
Cardiac, Pediatric plastic surgery
Heart models, birthmark removal via tissue expanders
Makerbot Replicator Z18
Denver University
Colorado, Denver
Cardiac Biomechanics Lab
heart models, bio printing research on artificial heart valves
BioBot 1
Erlanger
Medical Center
Tennessee, Chattanooga
Urology and other departments
Heart models, kidney tumor for patient education
Outsourcing 3D printing to Chattanooga based 3D Ops which uses the Stratasys Connex and other printers
Feinberg School of Medicine at Northwestern University
Illinois, Chicago
Pediatric Orthopedics, Radiology and General Surgery
Pediatric orthopedics and general surgical training
Unknown
Henry Ford Hospital
Michigan, Detroit
Cardiothoracic Surgery, Innovation Institute, Radiology
Heart models, transcatheter valve positioning, heart valve replacement planning
Unknown
Hospital for Sick Children
Ontario, Toronto
Pediatric Cardiology
Heart models for complex surgical training and patient education
Objet260 Connex
Houston Methodist
Texas, Houston
Neurosurgery, Cardiac Surgery, HM Research Institute
Heart models, bio printing research
MakerBot Replicator 2 and others
Jacobs Institute
New York, Buffalo
Neurosurgery, Biomedical Engineering
Brain vessel models, Vascular flow models
Stratasys Eden 260V
Kosair Children's Hospital
Kentucky, Louisville
Pediatric Cardiac Surgery
Heart models
Makerbot Replicator 2X
Lehigh Valley Health Network
Exploratory study
Not clear from reports whether program moved forward
Mayo Clinic
Minnesota, Rochester
Cardiac Surgery, General Surgery, Neurosurgery, Oncology, Oral and Maxillofacial Surgery, Orthopedic Surgery, Otorhinolaryngology, Pediatric Surgery, Plastic and Reconstructive Surgery, Radiology, Thoracic Surgery, Transplant Center, Urology, Vascular and Endovascular Surgery
Heart models, kidney models for renal sparing surgery, planning and simulation of complex endovascular aortic repair, patient-specific immobilization system for MRI, pre-operative bending for mandibular reconstruction, mirror image models for facial reconstruction, cutting guides for maxilla and mandibular reconstruction, templating and pre-bending in defect reconstruction in acetabular revision, guides for reverse shoulder arthroplasty, intraoperative localization and templating for orthopedic surgery, resection planning, custom osteotomy template,
Stratasys Connex 350 polyjet
Montefiore Medical Center, [University Hospital for Albert Einstein College of Medicine]
New York City
Pediatric Neurosurgery, Pediatric Rehabilitation, Craniofacial Surgery, Radiology, Plastic and Reconstructive Surgery
Cranial reconstruction for Craniosynostosis, Upper extremity prosthesis
Outsources cosmetic surgery models to Mirror Me 3D
Mount Sinai Hospital
Ontario, Toronto
Pathology, Institute of Biomaterials and Biomedical Engineering
Joint replacement
Unknown
Nemours / Alfred I. DuPont Hospital for Children
Delaware, Wilmington
Orthopedic Surgery
Pediatric prostheses
Stratasys Dimension 3D printer
New York- Presbyterian Morgan Stanley Children’s Hospital
New York City
Pediatric Cardiology
Pediatric heart models
Have outsourced printing to Materialise in past. Moved in-house?
Niklaus Children's Hospital
Florida, Miami
Pediatric Cardiology
Pediatric heart models
Stratasys Connex3
Phoenix Children's Hospital
Phoenix Arizona
Neurosurgery, Oncology, Cardiac
Heart models, brain tumors for “patient empowerment”
3D Systems ZCorp 650 and 3 others for different materials
Rady Children's hospital
California, San Diego
Pediatric Cardiac Surgery
heart models for planning complex heart surgeries and family education
Rady is outsourcing the printing of models to local providers.
Seattle Children's Hospital
Washington, Seattle
Cardiac Surgery, Oral and maxillofacial Surgery, Neurosurgery, Radiology
Heart models, cranium models
HeartMAP™ Simulator
Shriner’s Hospital for
Children
Texas, Houston
Orthopedic Surgery, Bioengineering students from Rice
prosthetic hands
Unknown
Shriners Hospital for Children
Illinois, Chicago
Craniomaxillofacial Surgery, Radiology, Pediatric Spine Surgery
Craniofacial reconstructions, cranial vault implant, cutting guides and templates, Spine models
Printing outsourced to the Jump Trading Simulation and Education Institute and Medical Modeling Inc.
Stanford Medical Center
[Note: This entry needs work; sources are less definitive than usual. Since Stanford is my alma mater, I hate to do it an injustice!]
California, Palo Alto
Orthopedic Surgery, Craniomaxillofacial Surgery
Pre-operative plate bending template, research on polymer-, ceramic-, hydrogel-based, and hybrid scaffolds with well-defined complex geometry and highly-reproducible controlled porous architecture.
3D Systems Projet and in-house fabrication system
St. Louis Children’s Hospital
Missouri, St. Louis
Cardiology
Heart models
3D Systems
University of Colorado School of Medicine
Colorado, Denver
Biomedical Lab
Metal parts for prosthetics
Germany-based EOS direct metal laser sintering printer.
University of Illinois College of Medicine
Illinois, Peoria
Craniofacial, Cardiac Surgery
Heart models
Printing outsourced to the Jump Trading Simulation and Education Institute
University of Michigan CS Mott Children’s Hospital
Michigan, Ann Arbor
Pediatric Surgery, Pediatric Otolaryngology, Biomedical Engineering
Implantable bioresorbable splint for tracheo-bronchomalacia, assessment of need for Ex Utero Intrapartum Treatment (EXIT) Procedure, 3D biomaterial printing
EOS Formiga P100 selective laser sintering building the splints with a polycaprolactone material (biodegradable polymer).
University of Pennsylvania Medical Center
Pennsylvania, Philadelphia
Maxillofacial, Orthopedic
Orthopedic implants
Unknown
University of Ottawa Hospital
[Need update from Frank Rybicki, MD]
Unknown
University of Toronto, Sunnybrook Health Sciences Centre
Ontario, Toronto
Plastic Surgery
skin bio printing for burn treatment
First gen prototype bio printer
University of Utah Health Sciences Center
Utah, Salt Lake City
Oncology
Prosthetic ear
Unknown
Wake Forest School of Medicine
North Carolina, Winston-Salem
Urology
Bio-printing of skin for burn treatment, research on printing of tissues and organs, regenerative medicine
Bespoke integrated tissue-organ printer (ITOP) which combines and layers hydrogels, human cells and biodegradable materials for structure.
Walter Reed National Military Medical Center, Medical Applications Center
Maryland, Bethesda
Craniofacial, Orthopedic, Dental, Radiology
Medical models, custom implants, surgical positioning, cutting and drill guides
3D Systems’ ZCorp 650 and 450, Arcam Electron Beam Melting (EBM), 3DS’ SLA 7000 and SLA 500, Viper Pro, Stratasys’ uPrint
Washington University School of Medicine
Missouri, St. Louis
Cardiothoracic Surgery, Otolaryngology
Heart models, prosthetic forearms and hands
Five printers including a BioBot.
Weill Cornell Medical College
New York City
Cardiothoracic Surgery
Research on bio-printing of heart valves, intervertebral disk repair
Makerbot Replicator 2, Stratasys uPrint and Fortus 250mc

 RSS Feed
RSS Feed